Introduction
Pneumothorax is air within the pleural space, causing lung collapse due to positive pleural pressure. Tension pneumothorax develops when this pressure is transmitted to the mediastinum (see Image. Left-Sided Tension Pneumothorax Radiograph). Although uncommon, this condition follows a malignant course and can result in death if untreated.[1][2] Tension pneumothorax may present in prehospital settings, emergency departments, and intensive care units.[3][4][5][6]
The thorax comprises 3 compartments: the right and left pulmonary cavities and the centrally located mediastinum. The parietal pleura lines the pulmonary cavities, while the visceral pleura envelops the lungs. The pleural cavity, a potential space between these pleurae, normally contains serous fluid that lubricates the pleural surfaces. During inspiration, diaphragmatic depression and outward rib movement expand the lungs, facilitated by a slightly negative pleural pressure. Expiration involves diaphragmatic elevation and slight inward rib movement, with positive pleural pressure driving air out of the lungs.
Disruption of the pleura can allow air to enter the pleural cavity. Elevated positive pleural pressure causes lung collapse, impairing oxygenation and ventilation of the affected lung. Excessive pleural pressure compresses mediastinal structures, including the heart, great vessels, and trachea. This process leads to tension pneumothorax, compromising respiration, venous return, and cardiac output. Early recognition and prompt management of tension pneumothorax are essential to prevent mortality. Proficiency in emergency thoracic decompression is a critical skill for all healthcare professionals.[7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Pneumothorax may be classified as traumatic or atraumatic. Outside the hospital, traumatic pneumothorax commonly results from penetrating or blunt trauma, rib fractures, or pulmonary decompression sickness.[8][9] Within the hospital setting, traumatic pneumothorax may develop iatrogenically as a complication of the following procedures:
- Central venous catheterization of the subclavian or internal jugular vein
- Lung biopsy
- Barotrauma from positive pressure ventilation
- Percutaneous tracheostomy
- Thoracentesis
- Pacemaker insertion
- Bronchoscopy
- Cardiopulmonary resuscitation
- Intercostal nerve block [10]
Atraumatic pneumothorax may be primary with an unknown cause or secondary to underlying lung disease. Recognition of both traumatic and atraumatic causes is essential, as tension pneumothorax can arise from any of these conditions or interventions, necessitating vigilance across clinical settings.
Epidemiology
The actual incidence of tension pneumothorax is difficult to determine, as many patients receive decompressive needle thoracotomy before arrival at trauma centers. Approximately 20% of those with trauma present with an associated pneumothorax or tension pneumothorax, with this rate rising to 50% in cases of severe chest trauma. The risk of traumatic pneumothorax depends on the injury's size and mechanism. A review of military deaths from thoracic trauma indicates that up to 5% of combat casualties have tension pneumothorax at the time of death.[11][12]
Traumatic and tension pneumothorax are more common than spontaneous pneumothorax. Tension pneumothorax develops in 1% to 2% of cases initially presenting as idiopathic spontaneous pneumothorax. Meanwhile, the rate of iatrogenic pneumothorax is increasing in hospitals globally due to greater reliance on positive-pressure ventilation (PPV) and central venous catheterization (CVC). Failed initial venous access, subclavian vein approaches, and PPV all correlate with increased pneumothorax risk.[13]
The risk of CVC-related pneumothorax rises when catheters are placed in the internal jugular or subclavian veins. Pneumothorax incidence following CVC ranges from approximately 1% to 13%, increasing as high as 30% under certain circumstances.[14] Use of ultrasound guidance reduces this risk. Iatrogenic pneumothorax typically causes significant morbidity but rarely results in death. The incidence has been reported at 5 to 7 per 10,000 hospital admissions. Results from a recent study found that 95% of pneumothorax episodes were iatrogenic. Barotrauma from mechanical ventilation accounted for 69.6% of cases, with 41.1% progressing to tension pneumothorax. CVC insertion was responsible for 13.2% of cases.[15]
Pathophysiology
Tension pneumothorax results from disruption of pleural cavity dynamics. Normally, pleural cavity pressure remains negative relative to lung and atmospheric pressures. The lung tends to recoil inward but remains expanded due to the chest wall’s outward recoil and the pleural pressure gradient. Pneumothorax develops when communication forms between the pleural cavity and the lung, allowing air to enter the cavity. This air accumulation increases pleural pressure, compressing the lung and impairing ventilation and oxygenation.[16]
Tension pneumothorax arises when air accumulation becomes sufficient to compress the mediastinum and shift it contralaterally (see Image. Left Tension Pneumothorax Radiograph). Compression of the superior vena cava impedes venous return, reducing cardiac output. Tracheal deviation results from mediastinal displacement.[17] Reduced cardiac output exacerbates hypoxemia by increasing pulmonary vascular resistance. Circulatory collapse may lead to acidosis and, if untreated, cardiac arrest.[18][19]
History and Physical
Tension pneumothorax is a medical emergency requiring immediate intervention. A rapid, focused examination typically reveals severe respiratory distress, hypotension, and an enlarged, hyperresonant hemithorax with absent breath sounds. Tracheal deviation and mediastinal shift toward the contralateral side may be evident. Air release confirms the diagnosis upon inserting a large-bore needle into the second intercostal space at the midclavicular line.
A detailed history often identifies the cause of tension pneumothorax. Recent trauma or medical procedures such as PPV or CVC are common antecedents. Underlying pulmonary conditions, such as asthma or pneumonia, may also contribute. In addition to dyspnea, patients frequently report sharp, pleuritic chest pain radiating to the ipsilateral back or shoulder.
Additional early physical signs include tachypnea, tachycardia, chest retractions, cyanosis, and jugular venous distension. The affected hemithorax demonstrates reduced tactile fremitus and hyperresonance on percussion. Subcutaneous emphysema may be present in some cases. Tension pneumothorax is a clinical diagnosis. Rapid deterioration and cardiac arrest can occur without immediate management.[20] Unconscious patients lacking respirations or a pulse require immediate resuscitation regardless of the underlying cause.
Evaluation
When the diagnosis is uncertain, the patient’s clinical status, whether stable or unstable, guides subsequent evaluation. Bedside ultrasound, when available, can confirm the diagnosis in hemodynamically unstable individuals. Concurrent stabilization and assessment of airway, breathing, and circulation remain priorities.
When performed by a skilled operator, ultrasound demonstrates 94% sensitivity and 100% specificity. Point-of-care ultrasound effectively detects pneumothorax, making it particularly useful in unstable individuals. Key ultrasound findings include the absence of lung sliding and the presence of a lung point.[21][22][23][24][25] Needle decompression should still be considered if diagnostic doubt persists after ultrasound examination.
Radiographic evaluation is recommended for hemodynamically stable patients (see Image. Right Tension Pneumothorax Radiograph). Initial assessment includes a chest x-ray to confirm the diagnosis.[26][27] Radiographic signs of pneumothorax include:
- Thin visceral pleural edge visible as a sharp line
- Absence of lung markings distal to the pleural edge
- Complete collapse of the ipsilateral lung
- Mediastinal shift away from the pneumothorax in tension pneumothorax
- Presence of subcutaneous emphysema
- Tracheal deviation toward the contralateral side in tension pneumothorax
- Flattening of the ipsilateral hemidiaphragm in tension pneumothorax
Chest computed tomography (CT) may be employed when the diagnosis on chest x-ray is uncertain. CT is the most definitive imaging modality for pneumothorax, but its routine use in tension pneumothorax is not recommended.
Treatment / Management
Tension pneumothorax may develop in any setting, and treatment depends on the circumstances at onset. Management typically occurs in the emergency department or intensive care unit. The patient’s hemodynamic stability guides strategies. Assessment of airway, breathing, and circulation is essential for all patients presenting with chest trauma. Penetrating chest wounds must be sealed using an airtight occlusive bandage covered by sterile plastic sheeting.
Administration of 100% supplemental oxygen reduces pneumothorax size by lowering alveolar nitrogen partial pressure. This intervention creates a diffusion gradient that accelerates nitrogen reabsorption and pneumothorax resolution. Only approximately 1.25% of the trapped air is absorbed without oxygen supplementation within 24 hours. PPV should be avoided initially, as it may exacerbate the tension pneumothorax. This treatment may be instituted after chest tube placement.[28][29](A1)
Immediate needle decompression must be performed without delay if the patient is hemodynamically unstable and clinical suspicion for pneumothorax is high. Needle placement is recommended at the second anterior intercostal space along the midclavicular line, inserted above the rib using an angiocatheter. When time permits, insertion at the fifth intercostal space along the anterior axillary line is preferred, as this location offers higher success rates and fewer complications. Long angiocatheters (>8 cm) are recommended to overcome chest wall thickness. Needle decompression allows reexpansion of the collapsed lung. However, rapid reexpansion may increase the risk of pulmonary edema. A chest x-ray and chest tube thoracostomy (CTT) should be obtained.[30]
Serial chest x-rays assist in monitoring pneumothorax resolution. Removal of the chest tube is appropriate once the lung has fully reexpanded, no air leaks are detected, and the patient demonstrates clinical improvement. Management of chest tubes is typically performed by experienced nurses, respiratory therapists, surgeons, and intensive care clinicians. CTT successfully resolves approximately 90% of pneumothorax cases. Video-assisted thoracoscopic surgery (VATS) or thoracotomy is reserved for cases unresponsive to CTT.[31][32][33][34](B2)
Surgical intervention is often indicated for patients with bilateral pneumothoraces, recurrent ipsilateral pneumothoraces, pulmonary decompression sickness, or persistent air leaks lasting more than 7 days. During VATS, mechanical or chemical pleurodesis is performed to prevent recurrence. Mechanical pleurodesis techniques include abrasion with scratchpads, dry gauze, or parietal pleura stripping. Chemical pleurodesis is an alternative for patients intolerant to mechanical methods and involves agents such as talc, minocycline, doxycycline, or tetracycline. Blood patch application has also demonstrated some efficacy. Endobronchial valve placement may be considered in cases of recurrent or unresolved pneumothorax. Results from recent studies indicate that pleurodesis significantly reduces the risk of pneumothorax recurrence; mechanical pleurodesis lowers this risk to less than 5%.[35][36](A1)
Differential Diagnosis
The differential diagnosis of tension pneumothorax includes the following:
- Pulmonary embolism
- Acute coronary syndrome
- Acute aortic dissection
- Myocardial infarction
- Pneumonia
- Acute pericarditis
- Rib fracture
- Diaphragmatic injuries
The combined physical findings of severe respiratory distress, hypotension, an enlarged hemithorax, ipsilaterally absent breath sounds, and contralateral tracheal deviation will distinguish tension pneumothorax from these conditions.
Prognosis
Tension pneumothorax may result from various causes and progresses rapidly to respiratory failure, cardiovascular collapse, and death if not promptly recognized and treated. Delays in diagnosis and intervention are strongly associated with poor outcomes. Uncomplicated pneumothorax may recur within 6 months to 3 years, with higher recurrence rates observed in individuals who smoke or have chronic obstructive pulmonary disease or acquired immunodeficiency syndrome.[37][38] Ventilator-associated tension pneumothorax carries a high risk of mortality and frequently proves fatal.[39] In contrast, procedure-related tension pneumothorax generally has a more favorable prognosis.[40]
Complications
Tension pneumothorax is life-threatening. In patients who survive this condition, complications may arise from the lung injury itself or CTT, which include the following:
- Pneumopericardium
- Pneumoperitoneum
- Hemothorax
- Bronchopulmonary fistula
- Damage to the neurovascular bundle during CTT
- Pain and skin infection at the CTT site
- Empyema
- Pyopneumothorax
Timely diagnosis and management help improve outcomes in patients with tension pneumothorax.
Consultations
Needle decompression may be performed by the clinician who detects the condition in a patient with respiratory distress and hypotension. After stabilizing the patient, one of the following specialists must be consulted for further evaluation and management:
- Thoracic surgeon
- Pulmonologist
- Interventional radiologist
- Intensivist
Early referral can help refine management strategies and improve outcomes.
Deterrence and Patient Education
Preventing tension pneumothorax involves minimizing risk factors predisposing individuals to this potentially fatal condition. Patient education must emphasize the following preventive strategies:
- Taking precautions during high-risk activities: Wearing seatbelts, adhering to speed limits, following workplace safety protocols, and using protective gear during sports can reduce trauma-related risk.
- Ensuring treatment compliance in chronic pulmonary conditions: Proper management of respiratory conditions, such as asthma and chronic obstructive pulmonary disease, lowers the risk of pneumothorax.
- Practicing safe ascent for divers and aviators: Gradual ascent prevents decompression sickness.[41] Additional precautions include avoiding alcohol before diving or flying, spacing out dives or flights, refraining from air travel shortly after a deep-sea dive, and maintaining good physical condition.
- Smoking cessation: Quitting smoking reduces the risk of lung pathology associated with spontaneous pneumothorax.
Patients should be advised to seek prompt medical attention for new or worsening symptoms, particularly after trauma. Although not all cases are preventable, adherence to these measures significantly lowers the risk of tension pneumothorax and its complications.
Pearls and Other Issues
The following are the key points in managing tension pneumothorax:
- Tension pneumothorax is a clinical diagnosis. The condition may arise from traumatic and atraumatic causes and prehospital and in-hospital settings.
- If a patient is hemodynamically unstable and a tension pneumothorax is likely, needle decompression must be performed immediately, followed by CTT.
- If the patient is stable, diagnostic imaging such as a chest x-ray may be obtained before treatment.
- Patients with pulmonary conditions predisposing them to high peak inspiratory pressures are at greater risk of tension pneumothorax.
- CTT suffices for managing most pneumothorax cases. Further surgical treatments, including VATS with pleurodesis, may be necessary in others.
Quick diagnosis and management can prevent significant morbidity and mortality from this condition.
Enhancing Healthcare Team Outcomes
Tension pneumothorax diagnosis and management require cooperation among interprofessional healthcare team members. The following comprise this team:
- First responders: These professionals are the first to identify the condition and perform needle decompression. The role varies by setting. Emergency medical technicians or designated physicians may respond in prehospital care. Emergency medicine clinicians take the lead in the emergency department. Intensivists respond in the intensive care unit.
- Nursing staff: Different nurses may be assigned to perform intravenous catheterization, initiate cardiac monitoring, and prepare the emergency cart while stabilizing a patient with tension pneumothorax. Once the patient is stable, nurses administer medications, coordinate care, and reinforce patient education.
- Radiologist: This clinician evaluates the extent of lung collapse or other associated injuries through imaging studies. The radiologist's role is critical to determining the definitive management of tension pneumothorax.
- Respiratory therapist: This healthcare professional assists in administering respiratory interventions like oxygen therapy and mechanical ventilation to patients with tension pneumothorax.
- Trauma or thoracic surgeon: CTT may be performed by an emergency clinician, trauma surgeon, or thoracic specialist. If pneumothorax does not resolve with CTT, a trauma or thoracic surgeon can perform another surgical procedure, like VATS, to correct the problem.
- Pulmonologist: This specialist renders care to patients on ventilatory support and manages the pulmonary conditions that may have caused the tension pneumothorax.
Collaboration and coordination among these interprofessional team members are crucial in prompt recognition, immediate intervention, and comprehensive management of tension pneumothorax.
Media
(Click Image to Enlarge)
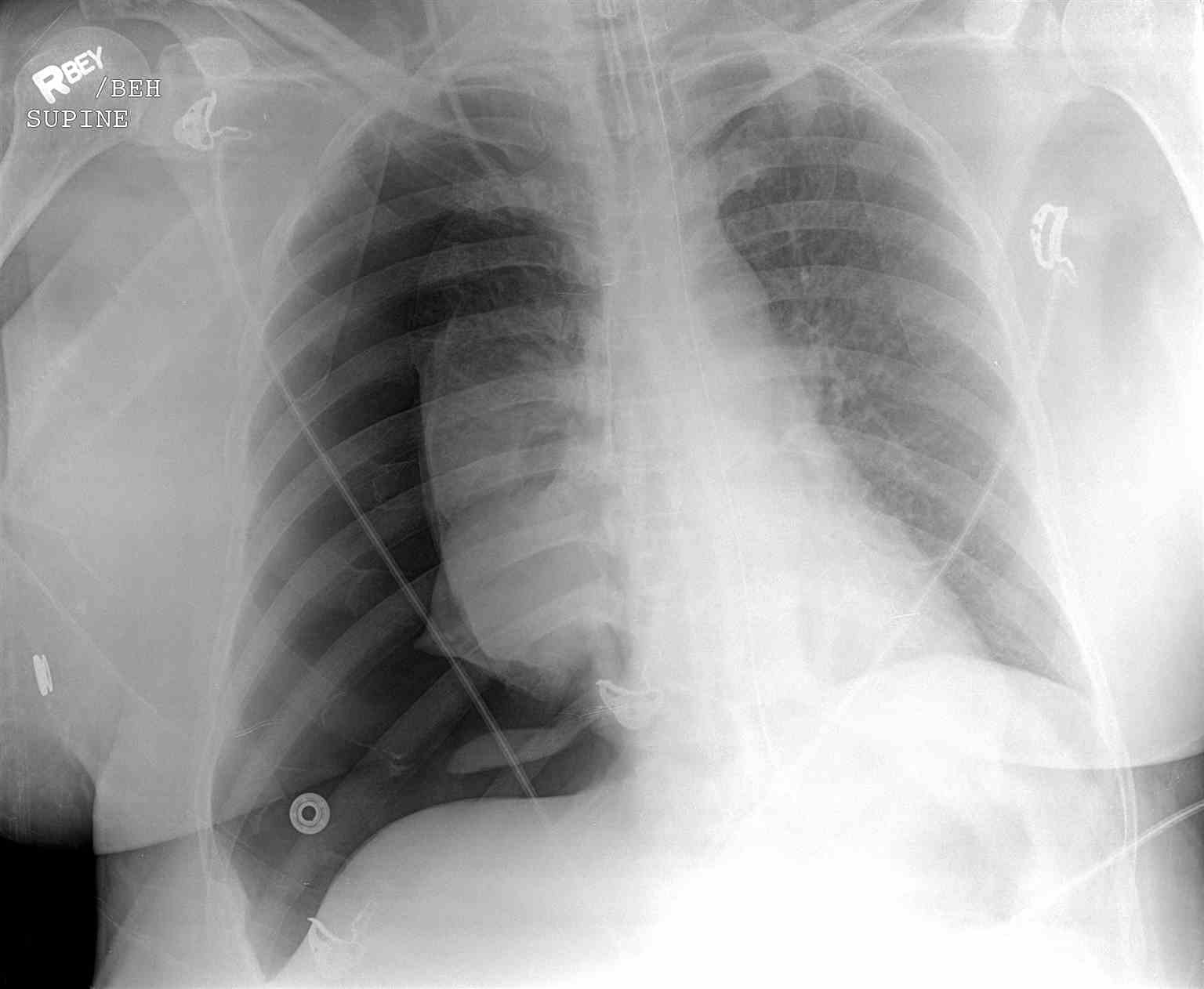
Right Tension Pneumothorax Radiograph. This image shows absent lung markings on the lateral side of the right pleural cavity and a collapsed right lung. The trachea and heart are displaced toward the left indicating a mediastinal shift.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
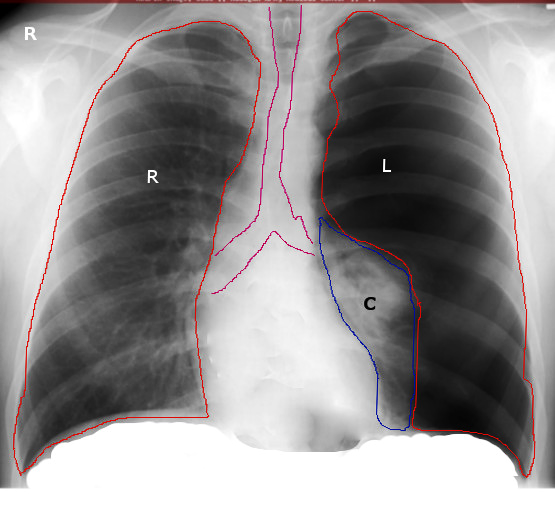
Left Tension Pneumothorax Radiograph. The left lung (marked "C") is collapsed, while the trachea and heart are displaced toward the right.
Image courtesy S.Bhimji MD
(Click Image to Enlarge)
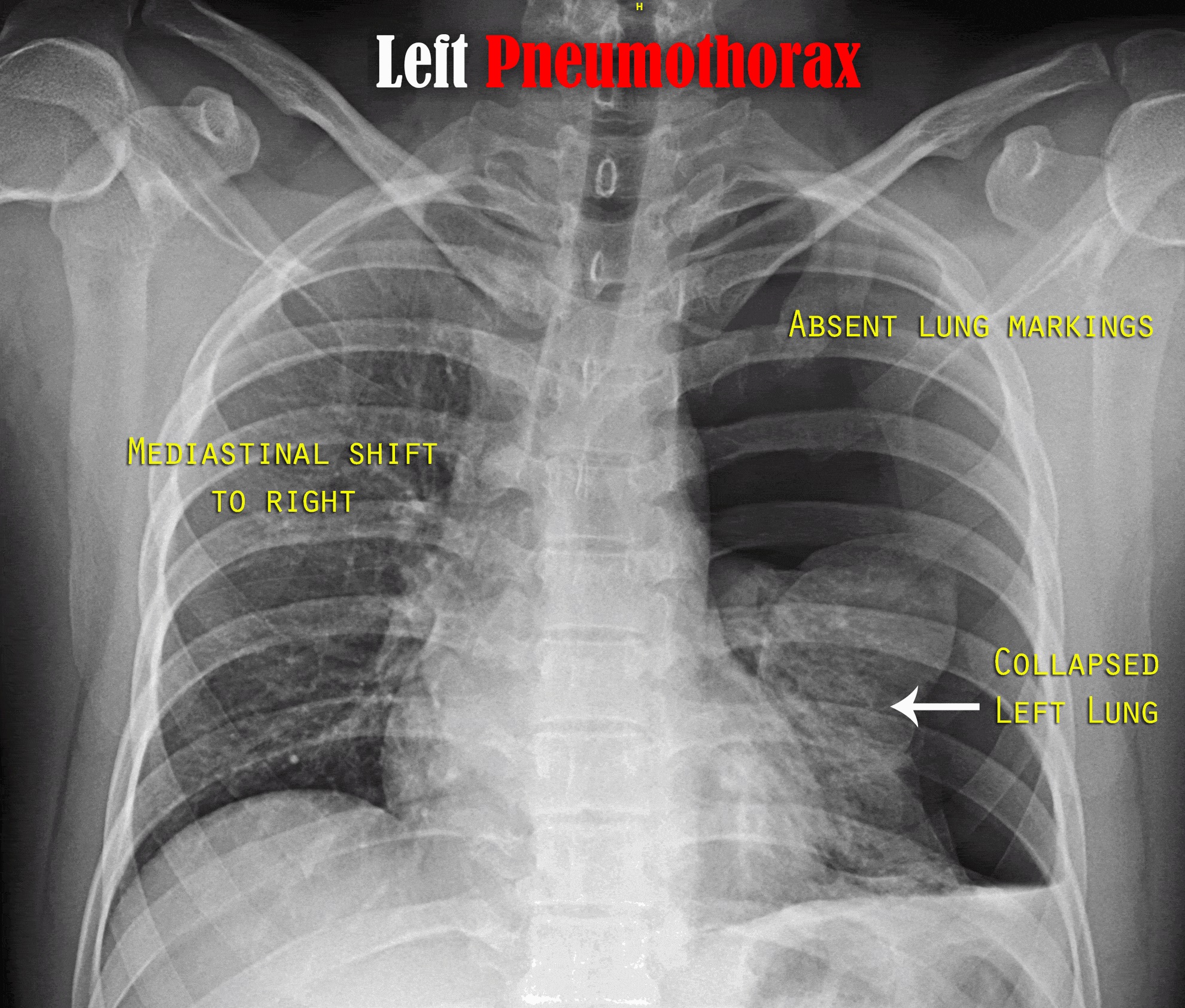
Left-Sided Tension Pneumothorax Radiograph. This image shows a collapsed left lung and mediastinal contents shifting to the right.
Karthik Easvur, Public Domain, via Wikimedia Commons
References
Rojas R, Wasserberger J, Balasubramaniam S. Unsuspected tension pneumothorax as a hidden cause of unsuccessful resuscitation. Annals of emergency medicine. 1983 Jun:12(6):411-2 [PubMed PMID: 6859647]
Level 3 (low-level) evidenceATLS Subcommittee, American College of Surgeons’ Committee on Trauma, International ATLS working group. Advanced trauma life support (ATLS®): the ninth edition. The journal of trauma and acute care surgery. 2013 May:74(5):1363-6. doi: 10.1097/TA.0b013e31828b82f5. Epub [PubMed PMID: 23609291]
Roberts DJ, Leigh-Smith S, Faris PD, Ball CG, Robertson HL, Blackmore C, Dixon E, Kirkpatrick AW, Kortbeek JB, Stelfox HT. Clinical manifestations of tension pneumothorax: protocol for a systematic review and meta-analysis. Systematic reviews. 2014 Jan 4:3():3. doi: 10.1186/2046-4053-3-3. Epub 2014 Jan 4 [PubMed PMID: 24387082]
Level 1 (high-level) evidenceCameron PA, Flett K, Kaan E, Atkin C, Dziukas L. Helicopter retrieval of primary trauma patients by a paramedic helicopter service. The Australian and New Zealand journal of surgery. 1993 Oct:63(10):790-7 [PubMed PMID: 8274122]
Coats TJ, Wilson AW, Xeropotamous N. Pre-hospital management of patients with severe thoracic injury. Injury. 1995 Nov:26(9):581-5 [PubMed PMID: 8550162]
Level 2 (mid-level) evidenceEckstein M, Suyehara D. Needle thoracostomy in the prehospital setting. Prehospital emergency care. 1998 Apr-Jun:2(2):132-5 [PubMed PMID: 9709333]
Diaz R, Heller D. Barotrauma and Mechanical Ventilation. StatPearls. 2025 Jan:(): [PubMed PMID: 31424810]
Melton LJ 3rd, Hepper NG, Offord KP. Incidence of spontaneous pneumothorax in Olmsted County, Minnesota: 1950 to 1974. The American review of respiratory disease. 1979 Dec:120(6):1379-82 [PubMed PMID: 517861]
Gupta D, Hansell A, Nichols T, Duong T, Ayres JG, Strachan D. Epidemiology of pneumothorax in England. Thorax. 2000 Aug:55(8):666-71 [PubMed PMID: 10899243]
Sharma A, Jindal P. Principles of diagnosis and management of traumatic pneumothorax. Journal of emergencies, trauma, and shock. 2008 Jan:1(1):34-41. doi: 10.4103/0974-2700.41789. Epub [PubMed PMID: 19561940]
Toffel M, Pin M, Ludwig C. [Thoracic Surgical Aspects of Seriously Injured Patients]. Zentralblatt fur Chirurgie. 2020 Feb:145(1):108-120. doi: 10.1055/a-0903-1461. Epub 2020 Feb 25 [PubMed PMID: 32097982]
McPherson JJ, Feigin DS, Bellamy RF. Prevalence of tension pneumothorax in fatally wounded combat casualties. The Journal of trauma. 2006 Mar:60(3):573-8 [PubMed PMID: 16531856]
Vinson DR, Ballard DW, Hance LG, Stevenson MD, Clague VA, Rauchwerger AS, Reed ME, Mark DG, Kaiser Permanente CREST Network Investigators. Pneumothorax is a rare complication of thoracic central venous catheterization in community EDs. The American journal of emergency medicine. 2015 Jan:33(1):60-6. doi: 10.1016/j.ajem.2014.10.020. Epub 2014 Oct 18 [PubMed PMID: 25455050]
Tsotsolis N, Tsirgogianni K, Kioumis I, Pitsiou G, Baka S, Papaiwannou A, Karavergou A, Rapti A, Trakada G, Katsikogiannis N, Tsakiridis K, Karapantzos I, Karapantzou C, Barbetakis N, Zissimopoulos A, Kuhajda I, Andjelkovic D, Zarogoulidis K, Zarogoulidis P. Pneumothorax as a complication of central venous catheter insertion. Annals of translational medicine. 2015 Mar:3(3):40. doi: 10.3978/j.issn.2305-5839.2015.02.11. Epub [PubMed PMID: 25815301]
El-Nawawy AA, Al-Halawany AS, Antonios MA, Newegy RG. Prevalence and risk factors of pneumothorax among patients admitted to a Pediatric Intensive Care Unit. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine. 2016 Aug:20(8):453-8. doi: 10.4103/0972-5229.188191. Epub [PubMed PMID: 27630456]
Roberts DJ, Leigh-Smith S, Faris PD, Blackmore C, Ball CG, Robertson HL, Dixon E, James MT, Kirkpatrick AW, Kortbeek JB, Stelfox HT. Clinical Presentation of Patients With Tension Pneumothorax: A Systematic Review. Annals of surgery. 2015 Jun:261(6):1068-78. doi: 10.1097/SLA.0000000000001073. Epub [PubMed PMID: 25563887]
Level 1 (high-level) evidenceMartin M, Satterly S, Inaba K, Blair K. Does needle thoracostomy provide adequate and effective decompression of tension pneumothorax? The journal of trauma and acute care surgery. 2012 Dec:73(6):1412-7. doi: 10.1097/TA.0b013e31825ac511. Epub [PubMed PMID: 22902737]
Level 3 (low-level) evidenceBarton ED, Rhee P, Hutton KC, Rosen P. The pathophysiology of tension pneumothorax in ventilated swine. The Journal of emergency medicine. 1997 Mar-Apr:15(2):147-53 [PubMed PMID: 9144053]
Level 3 (low-level) evidenceNelson D, Porta C, Satterly S, Blair K, Johnson E, Inaba K, Martin M. Physiology and cardiovascular effect of severe tension pneumothorax in a porcine model. The Journal of surgical research. 2013 Sep:184(1):450-7. doi: 10.1016/j.jss.2013.05.057. Epub 2013 Jun 5 [PubMed PMID: 23764307]
Level 3 (low-level) evidenceLight RW. Pleural diseases. Disease-a-month : DM. 1992 May:38(5):266-331 [PubMed PMID: 1572232]
Gordon R. The deep sulcus sign. Radiology. 1980 Jul:136(1):25-7 [PubMed PMID: 7384513]
DORNHORST AC, PIERCE JW. Pulmonary collapse and consolidation; the role of collapse in the production of lung field shadows and the significance of segments in inflammatory lung disease. The Journal of the Faculty of Radiologists. Faculty of Radiologists (Great Britain). 1954 Apr:5(4):276-81 [PubMed PMID: 24543591]
Zhang M, Liu ZH, Yang JX, Gan JX, Xu SW, You XD, Jiang GY. Rapid detection of pneumothorax by ultrasonography in patients with multiple trauma. Critical care (London, England). 2006:10(4):R112 [PubMed PMID: 16882338]
Soldati G, Iacconi P. The validity of the use of ultrasonography in the diagnosis of spontaneous and traumatic pneumothorax. The Journal of trauma. 2001 Aug:51(2):423 [PubMed PMID: 11493817]
Level 3 (low-level) evidenceShostak E, Brylka D, Krepp J, Pua B, Sanders A. Bedside sonography for detection of postprocedure pneumothorax. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2013 Jun:32(6):1003-9. doi: 10.7863/ultra.32.6.1003. Epub [PubMed PMID: 23716522]
Level 2 (mid-level) evidenceZarogoulidis P, Kioumis I, Pitsiou G, Porpodis K, Lampaki S, Papaiwannou A, Katsikogiannis N, Zaric B, Branislav P, Secen N, Dryllis G, Machairiotis N, Rapti A, Zarogoulidis K. Pneumothorax: from definition to diagnosis and treatment. Journal of thoracic disease. 2014 Oct:6(Suppl 4):S372-6. doi: 10.3978/j.issn.2072-1439.2014.09.24. Epub [PubMed PMID: 25337391]
Arao K, Mase T, Nakai M, Sekiguchi H, Abe Y, Kuroudu N, Oobayashi O. Concomitant Spontaneous Tension Pneumothorax and Acute Myocardial Infarction. Internal medicine (Tokyo, Japan). 2019 Apr 15:58(8):1131-1135. doi: 10.2169/internalmedicine.1422-18. Epub 2019 Jan 10 [PubMed PMID: 30626814]
Vallee P, Sullivan M, Richardson H, Bivins B, Tomlanovich M. Sequential treatment of a simple pneumothorax. Annals of emergency medicine. 1988 Sep:17(9):936-42 [PubMed PMID: 3137850]
Henry M, Arnold T, Harvey J, Pleural Diseases Group, Standards of Care Committee, British Thoracic Society. BTS guidelines for the management of spontaneous pneumothorax. Thorax. 2003 May:58 Suppl 2(Suppl 2):ii39-52 [PubMed PMID: 12728149]
Level 1 (high-level) evidenceDominguez KM, Ekeh AP, Tchorz KM, Woods RJ, Walusimbi MS, Saxe JM, McCarthy MC. Is routine tube thoracostomy necessary after prehospital needle decompression for tension pneumothorax? American journal of surgery. 2013 Mar:205(3):329-32; discussion 332. doi: 10.1016/j.amjsurg.2013.01.004. Epub [PubMed PMID: 23414956]
Terada T, Nishimura T, Uchida K, Hagawa N, Esaki M, Mizobata Y. How emergency physicians choose chest tube size for traumatic pneumothorax or hemothorax: a comparison between 28Fr and smaller tube. Nagoya journal of medical science. 2020 Feb:82(1):59-68. doi: 10.18999/nagjms.82.1.59. Epub [PubMed PMID: 32273633]
Chen KC, Chen PH, Chen JS. New options for pneumothorax management. Expert review of respiratory medicine. 2020 Jun:14(6):587-591. doi: 10.1080/17476348.2020.1740090. Epub 2020 Mar 15 [PubMed PMID: 32174202]
Eguchi M, Abe T, Tedokon Y, Miyagi M, Kawamoto H, Nakasone Y. [Traumatic Intercostal Lung Hernia Repaired by Video-assisted Thoracoscopic Surgery;Report of a Case]. Kyobu geka. The Japanese journal of thoracic surgery. 2019 Nov:72(12):1038-1041 [PubMed PMID: 31701918]
Level 3 (low-level) evidenceJohnson G. Traumatic pneumothorax: is a chest drain always necessary? Journal of accident & emergency medicine. 1996 May:13(3):173-4 [PubMed PMID: 8733651]
Level 2 (mid-level) evidencePaydar S, Ghahramani Z, Ghoddusi Johari H, Khezri S, Ziaeian B, Ghayyoumi MA, Fallahi MJ, Niakan MH, Sabetian G, Abbasi HR, Bolandparvaz S. Tube Thoracostomy (Chest Tube) Removal in Traumatic Patients: What Do We Know? What Can We Do? Bulletin of emergency and trauma. 2015 Apr:3(2):37-40 [PubMed PMID: 27162900]
van den Brande P, Staelens I. Chemical pleurodesis in primary spontaneous pneumothorax. The Thoracic and cardiovascular surgeon. 1989 Jun:37(3):180-2 [PubMed PMID: 2763278]
Level 1 (high-level) evidenceHuang TW, Lee SC, Cheng YL, Tzao C, Hsu HH, Chang H, Chen JC. Contralateral recurrence of primary spontaneous pneumothorax. Chest. 2007 Oct:132(4):1146-50 [PubMed PMID: 17550937]
Level 2 (mid-level) evidenceBritish Thoracic Society Fitness to Dive Group, Subgroup of the British Thoracic Society Standards of Care Committee. British Thoracic Society guidelines on respiratory aspects of fitness for diving. Thorax. 2003 Jan:58(1):3-13 [PubMed PMID: 12511710]
Level 1 (high-level) evidenceHsu CW, Sun SF, Lee DL, Chu KA, Lin HS. Clinical characteristics, hospital outcome and prognostic factors of patients with ventilator-related pneumothorax. Minerva anestesiologica. 2014 Jan:80(1):29-38 [PubMed PMID: 24122035]
Level 2 (mid-level) evidenceChen KY, Jerng JS, Liao WY, Ding LW, Kuo LC, Wang JY, Yang PC. Pneumothorax in the ICU: patient outcomes and prognostic factors. Chest. 2002 Aug:122(2):678-83 [PubMed PMID: 12171850]
Level 2 (mid-level) evidenceCooper JS, Hanson KC. Decompression Sickness. StatPearls. 2025 Jan:(): [PubMed PMID: 30725949]