Introduction
Drowning is defined as the process of developing respiratory impairment due to submersion or immersion in a liquid medium. Outcomes are categorized as death, morbidity, or no morbidity. The terms "wet drowning," "dry drowning," and "near-drowning" are no longer accepted, although they may appear in older literature.[1][2][3] Modern classification distinguishes between fatal drowning, which results in death, and nonfatal drowning, which results in survival with or without morbidity. (Sources: Hughes et al, 2025; Beerman et al, 2018)
Resuscitation may begin with in-water rescue breathing, which should be attempted only by trained rescuers when it can be performed safely. In this technique, the rescuer positions the victim face-up, opens the airway by extending the neck, seals their mouth over the victim’s nose, and delivers mouth-to-nose ventilations at a rate of about 12 to 16 breaths per minute for approximately 1 minute while swimming or moving toward a safe location. (Source: International Life Saving Federation, 2015) Chest compressions should continue in accordance with Basic Life Support (BLS) guidelines once both patient and rescuer reach a safe environment, such as dry land or a boat.[4]
Drowning is a major public health problem, particularly in children. Events usually occur rapidly and are most often silent. Thrashing movements are uncommon, and the typical presentation involves a motionless individual floating at the surface who then quickly disappears underwater.
Drowning occurs in both warm and cold water. Cold water can confer neuroprotection, especially in children. The greatest morbidity and mortality from nonfatal drowning result from tissue hypoxia, particularly cerebral hypoxia. Rapid correction of hypoxia is the highest priority in resuscitation. Survivors may still suffer severe neurologic sequelae, including persistent vegetative state, due to prolonged cerebral hypoxia.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Drowning results from accidental or intentional submersion in water or other liquids that impair oxygenation of tissues and organs.”[5][6][7] Risk factors include the following:
- Male sex
- African American race
- Age younger than 5 years
- Low socioeconomic status, often associated with limited access to swimming lessons [8]
- Alcohol consumption, associated with more than 50% of adult drowning cases
- Hypothermia
- Trauma
- Seizure disorders
- Neurodevelopmental conditions, including autism
- Risk-taking behaviors
- Panic attacks
- Acute medical emergencies, including myocardial infarction, cardiac arrhythmia, and hypoglycemia (Source: Briggs, 2025)
In infants, drowning is most often accidental and commonly occurs in bathtubs or even small containers such as bathing pails. Most infant deaths from this condition occur within 5 minutes of unsupervised exposure. Older children are more likely to drown in swimming pools, frequently when gates or fences are left unsecured. Adults more commonly drown in natural bodies of water such as lakes, rivers, or the sea. In many adult cases, drowning is associated with concurrent trauma, for example, cervical spine or head injury sustained while diving into shallow water.
Epidemiology
Drowning is the 3rd leading cause of death from unintentional injury worldwide, accounting for approximately 7% of such deaths.[9] The World Health Organization (WHO) estimates that 236,000 drowning-related deaths occur globally each year, a figure likely underestimated in developing countries. More than 90% of drowning fatalities occur in low- and middle-income regions.
In the U.S., the Centers for Disease Control and Prevention (CDC) identifies drowning as the most frequent cause of death in children 1 to 4 years of age. (Source: CDC Drowning Data, 2024) In children ages 5 to 14 years, drowning is the 2nd leading cause of unintentional injury death after motor vehicle crashes. (Source: CDC Drowning Facts, 2024)
A bimodal distribution is observed. The 1st peak involves children younger than 5 years who are unsupervised in pools or bathtubs, with fewer than 10% of these cases linked to abuse or neglect. The 2nd peak involves young individuals 15 to 30 years of age, most often during recreational swimming in natural bodies of water.
However, drowning has also become an emerging concern among older adults, particularly those with preexisting medical conditions such as cardiovascular or neurological disorders. Unintentional drowning in this population is often linked to reduced mobility, cognitive decline, polypharmacy, and comorbidities, which increase susceptibility to accidents. Intentional drowning may also occur, with mental and behavioral conditions contributing to suicide risk.[10]
For every fatal drowning, 4 nonfatal drowning cases require medical evaluation. Approximately 50% of these patients necessitate hospital admission and interventions.
Pathophysiology
An initial episode of panic disrupts normal breathing patterns and prompts struggling to remain above water. Involuntary inspiratory effort follows, leading to hypoxemia. Subsequent aspiration of fluid and reflex laryngospasm occur when water reaches the lower respiratory tract.
No significant difference exists between saltwater and freshwater drowning. Both result in hypoxemia and surfactant destruction, predisposing to noncardiogenic pulmonary edema and acute respiratory distress syndrome (ARDS). Cerebral edema and elevated intracranial pressure develop as consequences of cerebral hypoxia, which is the major contributor to morbidity and mortality.
Arrhythmias may occur secondary to hypoxemia and water-induced hypothermia. Although hypothermia can exert tissue-protective effects, it also increases the risk of cardiac dysrhythmias.
The 2 principal sequelae of drowning involve the cardiovascular and central nervous systems. Most patients lose consciousness within 2 minutes, and irreversible brain injury typically occurs within 4 to 6 minutes. Global central nervous system hypoperfusion triggers the release of excitotoxic neurotransmitters, free radicals, and lipid peroxidation. Cerebral edema with subsequent autonomic instability is frequently accompanied by ST-segment changes, reflecting stress-related myocardial injury. Hypoxemia also contributes to ventricular arrhythmias and severe pulmonary hypertension. Electrolyte disturbances are uncommon unless hypothermia is present.
History and Physical
Critical historical information is often provided by emergency medical services, family members, or bystanders who witnessed the submersion event. Key details include the estimated duration of submersion, length of rescue or extraction time, whether a pulse was lost, and whether rescue breathing or cardiopulmonary resuscitation (CPR) was initiated.
The clinical interview should be tailored to the patient’s age and circumstances. In neonates, questions may focus on maternal support at home, socioeconomic status, and maternal mental health to help distinguish accidental events from possible nonaccidental trauma. In children and adolescents, the history should explore swimming ability, possible alcohol involvement, and the likelihood of diving-related injuries associated with risk-taking behavior.
The secondary survey can proceed once primary stabilization and optimization of airway, breathing, and circulation are ensured. The assessment should include evaluation for traumatic injuries, particularly involving the head and neck, and removal of wet clothing to prevent exacerbation of hypothermia.
Evaluation
Drowning is primarily a clinical diagnosis. Laboratory and imaging studies are not routinely indicated in well-appearing, asymptomatic patients with normal oxygenation. When obtained, the diagnostic workup should be guided by history and physical examination.
Chest radiography is not universally required, and the initial study has limited correlation with clinical course or outcome. However, chest radiography and arterial blood gas analysis may be warranted for persistent hypoxemia or progressive respiratory symptoms.
For altered mental status, appropriate investigations include head computed tomography, blood glucose, arterial blood gas, toxicology screening, ethanol level, and metabolic panel. The most frequent laboratory abnormality is metabolic acidosis, typically due to lactic acidosis. Electrolyte disturbances are uncommon in nonfatal drowning.
Treatment / Management
Prehospital Resuscitation
Early management of drowning begins at the scene, prioritizing rescuer and patient safety with rapid extrication followed by immediate assessment of airway, breathing, and circulation. Since tissue hypoxia, especially cerebral hypoxia, is the principal determinant of morbidity and mortality in nonfatal drowning, airway and breathing take precedence over chest compressions. Rescue breaths should be initiated promptly for apneic patients, with supplemental oxygen administered if available. Current guidelines recommend 5 initial rescue breaths before chest compressions, contrasting with the usual 2 breaths in standard BLS.
In-water rescue breathing should only be performed by trained rescuers. This intervention interrupts progression to cardiac arrest but should be administered only when safe. The Heimlich maneuver is no longer recommended in drowning resuscitation.
Routine cervical spine immobilization is indicated only for patients with a history or signs of trauma, such as from diving or a fall. This targeted approach avoids delaying airway management and resuscitation in drowning victims without suspected spinal injury. Hypothermia should be addressed with passive measures, including insulating blankets and removal of wet clothing. Continuous monitoring of consciousness, respiratory effort, and pulse guides decisions for escalation.
Advanced prehospital interventions focus on maintaining oxygenation and hemodynamic stability. Acceptable measures include noninvasive positive-pressure ventilation and endotracheal intubation when airway protection is inadequate. Supraglottic airway devices are not recommended in drowning, as they provide less reliable airway protection and may increase aspiration risk. Cardiopulmonary monitoring and intravenous access allow early management of hypotension or arrhythmias. Patients with severe hypoxia or circulatory compromise should be transported rapidly to facilities capable of definitive care, including mechanical ventilation, advanced cardiovascular support, and extracorporeal life support if indicated. Early prehospital interventions aim to limit hypoxic injury and optimize outcomes, forming a critical bridge to subsequent in-hospital management.
Automated external defibrillators (AEDs) have a limited role in drowning resuscitation as shockable rhythms occur in only 2% to 12% of patients. AED application should not delay or interfere with rescue breaths and chest compressions, which remain the priority. When available, AEDs should be used promptly once CPR is underway, particularly if a primary cardiac cause is suspected, but ventilation and oxygenation are critical for successful resuscitation in drowning victims.
Hospital-Based Management
Upon arrival at the healthcare facility, management focuses on airway stabilization and optimization of oxygenation. Supplemental oxygen may initially be provided via nasal cannula or nonrebreather mask, with escalation to noninvasive positive-pressure ventilation or endotracheal intubation as indicated. Intubation is warranted when airway protection is inadequate or oxygenation cannot be maintained, defined as failure to achieve an oxygen saturation (SpO2) of 90% or greater despite high-flow oxygen. Oxygen should be titrated to maintain arterial saturation between 92% and 96% to avoid hypoxemia and hyperoxia. Nebulized bronchodilators may be administered for bronchospasm. Cardiac support should follow advanced cardiac life support (ACLS) protocols, and crystalloid infusion or vasopressors may be required for refractory hypotension.[11]
In hypothermic patients, pulse assessment should extend for 30 seconds because pulses may be weak, and inappropriate chest compressions in the presence of an organized rhythm may precipitate dysrhythmia. Careful treatment of individuals with hypothermia is essential to avoid arrhythmogenic stimulation. Both passive and active rewarming strategies should be implemented to restore core temperature.[12][13][14](B3)
Shivering can complicate drowning recovery by causing significant adverse effects, such as lactic acidosis, elevated intracranial pressure, rhabdomyolysis, discomfort, interference with monitoring devices, and increased metabolic demand and oxygen consumption. Management of shivering involves coordinated multimodal control as part of a shivering management protocol, including pharmacologic agents (eg, sedatives, analgesics, neuromuscular blockers) and surface warming tools (eg, heating blankets, forced air warmers), to prevent these complications and optimize patient comfort and stability during rewarming efforts.
Noncardiogenic pulmonary edema and ARDS may develop and should be managed with evidence-based supportive care. Glucocorticoids, diuretics, and empiric antibiotics are not recommended for routine use. Antibiotic therapy should be initiated only if clinical evidence of infection emerges. In hemodynamically unstable patients, extracorporeal membrane oxygenation may be considered as salvage therapy for refractory hypoxemia or severe hypothermia. Therapeutic hypothermia has also been investigated as a potential adjunctive treatment.
Differential Diagnosis
The differential diagnosis of drowning must remain broad, as several medical and traumatic pathologies can either mimic or precipitate submersion events. Inclusion of these etiologies ensures that potentially life-threatening but reversible causes are not overlooked during initial evaluation. The following conditions should be considered:
- Cardiac arrhythmia
- Hypoglycemia
- Head trauma
- Cervical spine trauma
- Suicide
- Homicide
- Seizure
- Chronic obstructive pulmonary disease exacerbation
- Congestive heart failure exacerbation
Diagnostic uncertainty often arises when submersion injury coexists with or masks other acute conditions. Structured history-taking, targeted imaging, and laboratory testing help clinicians navigate these challenges effectively.
Staging
Several classification systems are used to categorize drowning events based on clinical signs and outcomes. Of these methods, the Szpilman Drowning Severity Grades and the WHO's Nonfatal Drowning Categorization Framework (NDCF) are the most widely referenced, reflecting complementary applications in clinical management and public health surveillance.
The Drowning Severity Grades, originally proposed by Szpilman in 1997, provide a practical clinical tool to categorize drowning victims based on respiratory and circulatory signs. This system ranges from mild to severe presentations, correlating closely with mortality risk. The classification, outlined in Table 1, guides prognosis and treatment decisions for drowning patients and is widely adopted in both military and civilian settings.
Table 1. Szpilman Drowning Severity Grades
|
Severity Grade |
Clinical Signs |
Mortality |
|
1 |
Cough |
0% |
|
2 |
Rales |
1% |
|
3 |
Pulmonary edema |
4%-5% |
|
4 |
Pulmonary edema + shock |
18%-22% |
|
5 |
Apnea + pulse |
31%-44% |
|
6 |
Apnea without pulse |
88%-93% |
The WHO's NDCF is a comprehensive tool designed to classify nonfatal drowning cases based on the severity of respiratory impairment and the level of morbidity at the time of assessment. This framework, found in Table 2 below, provides mutually exclusive and standardized categories to improve data consistency, surveillance, and comparability across different settings globally.
Table 2. Nonfatal Drowning Categorization Framework
|
Severity of Respiratory Impairment After the Drowning Process Stopped |
Morbidity Category (Based on Decline from Previous Functional Capacity) at Time of Measurement |
|
(1) Mild impairment: Breathing; involuntary distressed coughing; fully alert |
(A) No morbidity: No decline |
|
(2) Moderate impairment: Difficulty breathing and/or disoriented but conscious |
(B) Some morbidity: Some decline |
|
(3) Severe impairment: Not breathing and/or unconscious |
(C) Severe morbidity: Severe decline |
The term “involuntary distressed coughing” describes the reflexive expulsion of liquid from the airway, which may be sustained, and was selected by the Working Group on Nonfatal Drowning as the most consistent indicator that drowning has begun across different settings. “Previous functional capacity” refers to the individual’s baseline cognitive, motor, and psychological abilities prior to the drowning event.
Key differences between these frameworks lie in their focus and application. The Szpilman grades emphasize clinical signs and mortality risk, guiding immediate patient management and prognosis. In contrast, the NDCF assesses respiratory impairment and subsequent functional decline, supporting public health monitoring and long-term outcome evaluation. Together, these systems provide complementary perspectives on drowning, addressing both acute clinical care and population-level surveillance.
Prognosis
Prompt recognition and appropriate management, including airway support, oxygenation, and early resuscitation, are critical to mitigating morbidity and improving survival outcomes. Individuals who are alert or only mildly confused at presentation generally have a favorable prognosis, whereas comatose patients typically experience poor outcomes. Individuals resuscitated with CPR often sustain severe brain injury and hypoxic encephalopathy. Hypoxemia after drowning is strongly associated with poor outcomes, and survivors frequently develop persistent neurological sequelae, contributing to long-term morbidity. Among children with brain injury, 10% to 30% require long-term rehabilitation, although hypothermia may confer some neuroprotective benefit in pediatric patients.
Complications
Drowning can result in a spectrum of complications ranging from mild to severe. Common, mild effects include coughing, respiratory distress, and laryngospasm, which may resolve with observation and supportive care. Uncommon but severe complications include hypoxic-ischemic brain injury, ARDS, pneumonia, and cardiac dysfunction, including arrhythmias and decreased cardiac output. The severity often correlates with submersion duration and the volume of aspirated water.
In severe drowning, hypoxia and hypoperfusion can trigger systemic inflammatory response, causing isolated cardiac, renal, or hepatic dysfunction, sepsis, or multiorgan failure. Rarely, victims with normal initial chest radiography may develop fulminant pulmonary edema within 12 hours, potentially reflecting delayed ARDS, neurogenic edema, or airway hyperreactivity.
Death from drowning primarily results from hypoxemia caused by water aspiration, which disrupts alveolar gas exchange, destroys surfactant, and produces noncardiogenic pulmonary edema. If rescue does not occur, hypoxia rapidly leads to loss of consciousness, apnea, and hypoxic cardiac arrest, usually presenting with bradycardia or pulseless electrical activity. Thus, early deaths are respiratory and cardiac in origin. Late deaths mainly arise from neurologic injury due to prolonged cerebral hypoxia, with most long-term sequelae or fatalities in patients who remain comatose after resuscitation. Secondary complications, including infection, multiorgan dysfunction, or delayed pulmonary edema, may also contribute to mortality.[15][16]
Deterrence and Patient Education
The Drowning Chain of Survival emphasizes prevention and timely intervention to reduce morbidity and mortality (see Image. Drowning Chain of Survival). First, primary prevention, including pool fencing, lifejacket use, swimming instruction, and vigilant supervision, addresses the root cause. Second, early recognition of distress and prompt activation of rescue services enable rapid professional response despite the often silent presentation of drowning. Third, provision of flotation from a safe distance (for example, throwing flotation or using a reaching device) prevents further submersion while minimizing risk to rescuers.
Fourth, extrication should occur only when safe. An extraction technique should be selected that preserves airway patency (near-horizontal with the head elevated for suspected shock or arrest, or a more vertical position if conscious and at risk for emesis), and delays should be avoided. Fifth, BLS should be initiated immediately, escalated to ACLS as indicated, and emergency department transport should be arranged for all patients receiving any resuscitative intervention.
Prevention remains the most effective intervention. As mentioned, most drowning events are avoidable. Primary preventive measures such as adequate supervision, swimming instruction, safety technology, regulation, and public education significantly reduce the risk of drowning-related morbidity and mortality. Infants and children should never be left unsupervised near water, and children should consistently wear life vests when swimming. Caregivers should be trained in CPR and advised to implement environmental safety measures such as gated pool enclosures. Alcohol and recreational drug use near water should be strictly avoided. Fewer than 6% of individuals rescued by lifeguards require hospital-based medical care. Education is critical to reducing drowning-related morbidity and mortality.[17]
Pearls and Other Issues
Patients with mild or no symptoms may be observed in the emergency department for 4 to 8 hours. These individuals may be discharged with appropriate return precautions if they remain clinically stable. Symptomatic patients require extended observation and may need admission to the hospital ward or intensive care unit, depending on symptom severity. Duration of submersion is the most critical determinant of survival, with markedly increased mortality when submersion exceeds 5 minutes.
Enhancing Healthcare Team Outcomes
The management of drowning requires an interprofessional team. This team is composed of the emergency department physician as leader, supported by physician assistants, nurse practitioners, nurses, respiratory therapists, and emergency medical services personnel, as well as intensivists and pediatricians when care involves critically ill or pediatric patients.
Initial management may involve oxygen delivery devices such as a nasal cannula, simple face mask, or nonrebreather mask. Depending on the severity of hypoxemia, noninvasive ventilation or endotracheal intubation may be required. Oxygen should be titrated to maintain oxygen saturation between 92% and 96% while avoiding hyperoxia. Nebulized albuterol may be administered for bronchospasm.
Respiratory therapists assist in monitoring the patient’s response to oxygen therapy and pharmacologic interventions, coordinating with the physician to optimize airway and ventilatory status. ACLS protocols should guide management if cardiac arrest occurs. Infusion of crystalloids and, when necessary, vasopressors, may be required to treat refractory hypotension.
Media
(Click Image to Enlarge)
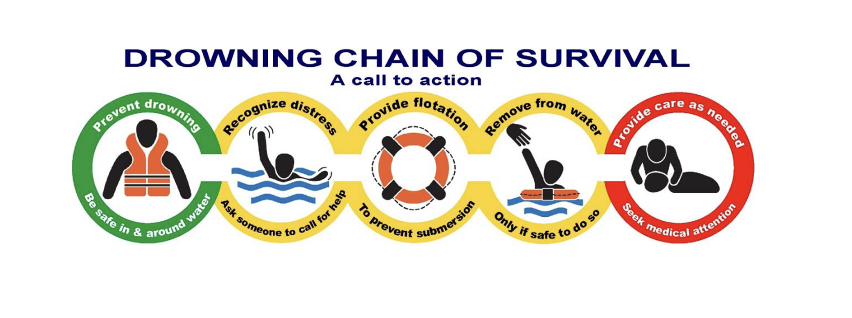
Drowning Chain of Survival. This schematic representation emphasizes prioritized sequential actions—from prevention and early recognition to bystander rescue, effective resuscitation, postresuscitation care, and rehabilitation—designed to improve outcomes in drowning incidents.
https://publications.aap.org/pediatrics/article/154/6/e2024068444/199870/2024-American-Heart-Association-and-American?autologincheck=redirected
References
Beck B, Smith K, Mercier E, Bernard S, Jones C, Meadley B, Clair TS, Jennings PA, Nehme Z, Burke M, Bassed R, Fitzgerald M, Judson R, Teague W, Mitra B, Mathew J, Buck A, Varma D, Gabbe B, Bray J, McLellan S, Ford J, Siedenburg J, Cameron P. Potentially preventable trauma deaths: A retrospective review. Injury. 2019 May:50(5):1009-1016. doi: 10.1016/j.injury.2019.03.003. Epub 2019 Mar 7 [PubMed PMID: 30898389]
Level 2 (mid-level) evidenceCoulthard MG, Varghese V, Harvey LP, Gillen TC, Kimble RM, Ware RS. A review of children with severe trauma admitted to pediatric intensive care in Queensland, Australia. PloS one. 2019:14(2):e0211530. doi: 10.1371/journal.pone.0211530. Epub 2019 Feb 7 [PubMed PMID: 30730910]
Nathanson A. Sailing Injuries: A Review of the Literature. Rhode Island medical journal (2013). 2019 Feb 1:102(1):23-27 [PubMed PMID: 30709070]
Goyal A, Singh B, Patel PH. Cardiopulmonary Resuscitation. StatPearls. 2025 Jan:(): [PubMed PMID: 29261985]
Adeloye D, Bowman K, Chan KY, Patel S, Campbell H, Rudan I. Global and regional child deaths due to injuries: an assessment of the evidence. Journal of global health. 2018 Dec:8(2):021104. doi: 10.7189/jogh.08.021104. Epub [PubMed PMID: 30675338]
Yeargin S. Leading Causes of Fatal and Nonfatal Unintentional Injury for Children and Teens and the Role of Lifestyle Clinicians: A Commentary. American journal of lifestyle medicine. 2019 Jan-Feb:13(1):26-29. doi: 10.1177/1559827618805414. Epub 2018 Dec 29 [PubMed PMID: 30627072]
Level 3 (low-level) evidenceLeth PM. Homicide by drowning. Forensic science, medicine, and pathology. 2019 Jun:15(2):233-238. doi: 10.1007/s12024-018-0065-9. Epub 2019 Jan 5 [PubMed PMID: 30612261]
Dezfulian C, McCallin TE, Bierens J, Dunne CL, Idris AH, Kiragu A, Mahgoub M, Shenoi RP, Szpilman D, Terry M, Tijssen JA, Tobin JM, Topjian AA. 2024 American Heart Association and American Academy of Pediatrics Focused Update on Special Circumstances: Resuscitation Following Drowning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2024 Dec 3:150(23):e501-e516. doi: 10.1161/CIR.0000000000001274. Epub 2024 Nov 12 [PubMed PMID: 39530204]
McCallin TE, Dezfulian C, Bierens J, Dunne CL, Idris AH, Kiragu A, Mahgoub M, Shenoi RP, Szpilman D, Terry M, Tijssen JA, Tobin JM, Topjian AA. 2024 American Heart Association and American Academy of Pediatrics Focused Update on Special Circumstances: Resuscitation Following Drowning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Pediatrics. 2024 Dec 1:154(6):. pii: e2024068444. doi: 10.1542/peds.2024-068444. Epub [PubMed PMID: 39530213]
Peden AE, Taylor DH, Franklin RC. Pre-Existing Medical Conditions: A Systematic Literature Review of a Silent Contributor to Adult Drowning. International journal of environmental research and public health. 2022 Jul 21:19(14):. doi: 10.3390/ijerph19148863. Epub 2022 Jul 21 [PubMed PMID: 35886717]
Level 1 (high-level) evidenceFulton II MR, Nordquist E. Advanced Cardiac Life Support (ACLS). StatPearls. 2025 Jan:(): [PubMed PMID: 40198051]
Cimpoesu D, Corlade-Andrei M, Popa TO, Grigorasi G, Bouros C, Rotaru L, Nedelea PL. Cardiac Arrest in Special Circumstances-Recent Advances in Resuscitation. American journal of therapeutics. 2019 Mar/Apr:26(2):e276-e283. doi: 10.1097/MJT.0000000000000927. Epub [PubMed PMID: 30839376]
Level 3 (low-level) evidenceWebber J, Moran K, Cumin D. Paediatric cardiopulmonary resuscitation: Knowledge and perceptions of surf lifeguards. Journal of paediatrics and child health. 2019 Feb:55(2):156-161. doi: 10.1111/jpc.14097. Epub 2018 Jun 26 [PubMed PMID: 29943876]
Parenteau M, Stockinger Z, Hughes S, Hickey B, Mucciarone J, Manganello C, Beeghly A. Drowning Management. Military medicine. 2018 Sep 1:183(suppl_2):172-179. doi: 10.1093/milmed/usy136. Epub [PubMed PMID: 30189074]
Szpilman D, Morgan PJ. Management for the Drowning Patient. Chest. 2021 Apr:159(4):1473-1483. doi: 10.1016/j.chest.2020.10.007. Epub 2020 Oct 14 [PubMed PMID: 33065105]
Berger S, Siekmeyer M, Petzold-Quinque S, Kiess W, Merkenschlager A. Drowning and Nonfatal Drowning in Children and Adolescents: A Subsequent Retrospective Data Analysis. Children (Basel, Switzerland). 2024 Apr 6:11(4):. doi: 10.3390/children11040439. Epub 2024 Apr 6 [PubMed PMID: 38671656]
Level 2 (mid-level) evidenceDenny SA, Quan L, Gilchrist J, McCallin T, Shenoi R, Yusuf S, Hoffman B, Weiss J, COUNCIL ON INJURY, VIOLENCE, AND POISON PREVENTION. Prevention of Drowning. Pediatrics. 2019 May:143(5):. pii: e20190850. doi: 10.1542/peds.2019-0850. Epub 2019 Mar 15 [PubMed PMID: 30877146]