 Anatomy, Shoulder and Upper Limb, Hand Dorsal Interossei Muscle
Anatomy, Shoulder and Upper Limb, Hand Dorsal Interossei Muscle
Introduction
The dorsal interosseous muscles are paired intrinsic muscles of the hand situated between the metacarpals (see Image. Dorsal Interossei of the Hand). This group consists of 4 muscles responsible for finger abduction. These muscles also contribute to flexion at the metacarpophalangeal (MCP) joints and extension at the interphalangeal joints. All interossei receive innervation from the deep branch of the ulnar nerve. Injury to this nerve can significantly impair intrinsic hand function, particularly finger abduction and adduction, which depend primarily on the interossei.[1]
Understanding the anatomy and physiology of the dorsal interosseous muscles aids in diagnosing ulnar nerve injuries and evaluating hand dysfunction. Precise knowledge of these muscles supports surgical planning for procedures involving the metacarpals, tendon repairs, and nerve decompression. Palpation and functional testing of the interossei provide valuable insight during clinical examinations, particularly in cases of trauma or neuropathy. Mastery of interosseous muscle mechanics enhances outcomes in reconstructive and rehabilitative hand surgery.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Among the intrinsic hand muscles, the dorsal interossei occupy the most dorsal position (see Image. Dorsal Interossei on Magnetic Resonance Imaging). These bipennate muscles serve as primary abductors of the 2nd, 3rd, and 4th digits at the MCP joints and assist with flexion at the MCP joints and extension at the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints.
The 1st dorsal interosseous muscle originates from the adjacent surfaces of the 1st and 2nd metacarpals and inserts into the lateral base of the 2nd phalanx and extensor hood of the 2nd digit.[2] The 2nd dorsal interosseous muscle arises from the medial aspect of the 2nd metacarpal and lateral aspect of the 3rd metacarpal, inserting into the lateral base of the 3rd phalanx and corresponding extensor hood.
The 3rd dorsal interosseous muscle originates from the medial portion of the 3rd metacarpal and lateral portion of the 4th metacarpal, with insertion at the medial base of the 3rd phalanx and extensor hood of the 3rd digit. The 4th dorsal interosseous muscle arises from the lateral aspect of the 4th metacarpal and medial side of the 5th metacarpal, inserting into the lateral base of the 4th phalanx and extensor hood of the 4th digit.
Embryology
At the end of the 4th week of embryonic development, 4 limb buds emerge from the somites and mesenchyme of the lateral plate mesoderm, covered by ectoderm.[3] The development of the upper extremities is driven by several protein factors, with fibroblast growth factors (FGFs) and Sonic Hedgehog (Shh) playing key roles. The expression and interactions of these proteins contribute to the formation of 3 spatial limb axes: proximodistal, anteroposterior, and dorsoventral.[4]
Hand development begins with the flattening of the distal upper extremity buds around days 34 to 38 of embryonic development. Somites form the limb musculature, while mesenchyme from the lateral plate mesoderm gives rise to bone and cartilage. The somitic mesoderm of the hand divides into superficial and deep layers. Both the palmar and dorsal interossei develop from the deep layer of this mesoderm. By the 12th week, tendons are fully formed and functional.[5]
Blood Supply and Lymphatics
The 1st dorsal interosseous muscle receives its vascular supply from the 1st dorsal metacarpal artery, which originates directly from the radial artery. The 2nd, 3rd, and 4th dorsal interossei are supplied by the 2nd, 3rd, and 4th dorsal metacarpal arteries, which arise from the dorsal carpal arch. All dorsal metacarpal arteries bifurcate into their respective dorsal digital arteries and anastomose with the common palmar digital arteries (see Image. Arteries of the Hand).[6]
Venous blood from the fingers drains into the digital palm, dorsal digital, and intercapitular veins, forming a complex vascular network. These veins transport blood through the superficial palmar venous arc and the dorsal venous arc, both of which communicate with the ulnar, cephalic, and basilic veins.
Lymphatic drainage of the upper limbs is divided into superficial and deep systems. Lymphatic plexuses in the skin of the palm and dorsum of the hand ascend with the cephalic and basilic veins toward the axillary and cubital lymph nodes, respectively. Deep lymphatic vessels follow the primary deep veins and ultimately drain into the humeral lymph nodes.[7]
Nerves
The deep branch of the ulnar nerve supplies both the palmar and dorsal interossei. This nerve derives from the nerve roots of C8 and T1, with T1 being the major innervating segment (see Image. Ulnar Nerve Pathway).[8][9]
Physiologic Variants
Classically, students are taught that all dorsal interossei have 2 heads, termed "bipennate." However, a retrospective study found that approximately 25% of dorsal interossei are unipennate.[10] The study also concluded that traditional teachings have oversimplified the attachment sites of both palmar and dorsal interossei, which exhibit significant variability.[11] These distal attachment sites include bony attachments, the volar plate, and portions of the extensor hood.
Surgical Considerations
Treatment for metacarpal fractures typically involves hand surgery, with metacarpal shortening ranging from 2 mm to 10 mm.[12] Researchers have found that a 2-mm shortening reduces the strength of the respective interossei by approximately 8%.[13]
Compartment syndromes of the interossei are uncommon and difficult to diagnose due to their atypical presentations. These conditions generally occur in patients who have experienced crush injuries, burns, or severe ischemia. A case report described a 1st dorsal interosseous compartment syndrome in a teacher, likely caused by overuse injury from writing. This injury went undiagnosed for 8 years and was relieved through simple tendon sheath decompression.[14]
Clinical Significance
The dorsal interossei receive innervation from the deep palmar branch of the ulnar nerve. Injury to the ulnar nerve can lead to weakness or even atrophy of the interossei, typically caused by nerve root impingement, brachial plexus compression, or nerve entrapment at the elbow, forearm, or wrist. Ulnar nerve entrapment is the 2nd most common form of neuropathy seen in patients.[15]
Depending on which nerve fibers are affected, patients may experience weakness in finger abduction. While the lumbricals are the primary contributors to flexion at the MCP joints and extension at the DIP and PIP joints, the interossei also play a minor role in these movements. A late manifestation of ulnar nerve injury, the ulnar claw hand deformity, results from weakness in the 3rd and 4th lumbricals, as well as the interossei. This condition causes weakness in the extension of the 4th and 5th MCP joints and flexion of the 4th and 5th PIP and DIP joints.[16]
Several clinical examinations are used to assess ulnar nerve function. Clinicians can evaluate the dorsal interossei by instructing patients to abduct their 2nd through 5th digits against resistance. Weakness in this action would indicate an ulnar nerve injury.
Media
(Click Image to Enlarge)
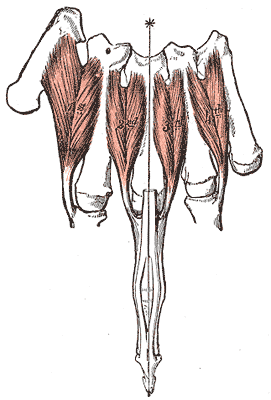
Dorsal Interossei of the Hand. Superior view illustrating the dorsal interossei muscles and their anatomical positioning between the metacarpal bones.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
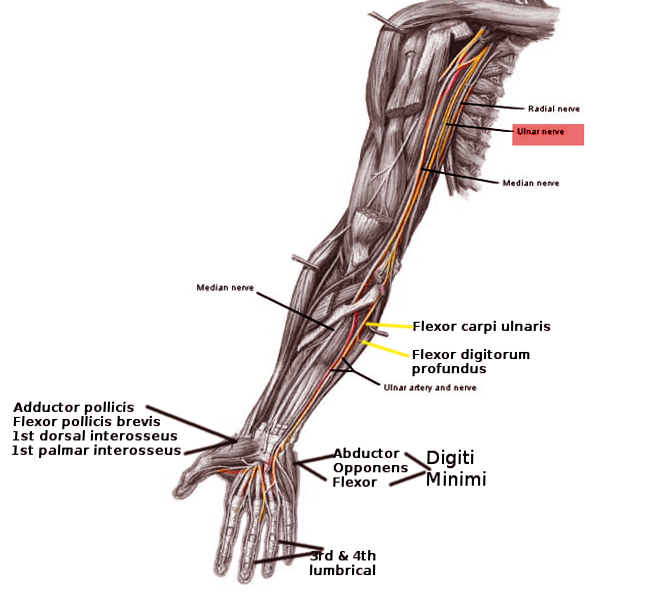
Ulnar Nerve Pathway. Anterior view illustrating the course of the ulnar nerve from the shoulder to the hand.
Image courtesy O.Chaigasame
(Click Image to Enlarge)
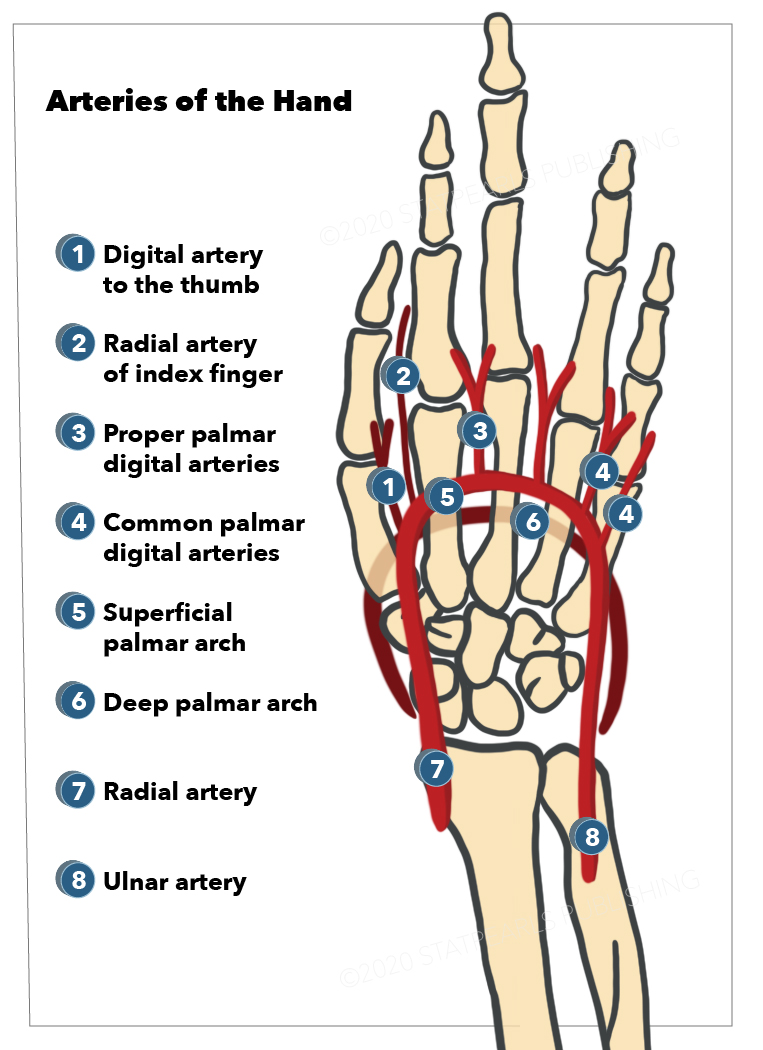
Arteries of the Hand. Shown here are the ulnar artery, radial artery, deep palmar arch, superficial palmar arch, common palmar digital arteries, proper palmar digital arteries, radial artery of the index finger (radialis indicis), and digital artery to the thumb (princeps pollicis).
StatPearls Publishing Illustration
(Click Image to Enlarge)
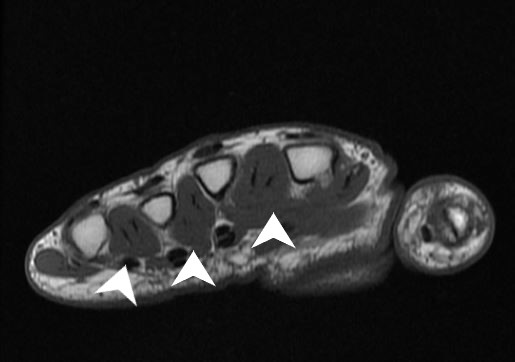
Dorsal Interossei on Magnetic Resonance Imaging. Cross-sectional view of a prone hand, showing the dorsal interossei (white arrows) from an anterior perspective.
Contributed by Dawood Tafti, MD.
References
Picasso R, Zaottini F, Pistoia F, Perez MM, Macciò M, Bianco D, Rinaldi S, Pansecchi M, Rossi G, Tovt L, Martinoli C. Ultrasound of the palmar aspect of the hand: normal anatomy and clinical applications of intrinsic muscles imaging. Journal of ultrasonography. 2023 Sep:23(94):e122-e130. doi: 10.15557/jou.2023.0021. Epub 2023 Sep 11 [PubMed PMID: 37732107]
Low ZX, McGrouther DA. First dorsal interosseous muscle reconstruction: a systematic review of its attachments. Surgical and radiologic anatomy : SRA. 2023 Jul:45(7):901-909. doi: 10.1007/s00276-023-03149-0. Epub 2023 May 12 [PubMed PMID: 37169993]
Level 1 (high-level) evidenceTickle C. How the embryo makes a limb: determination, polarity and identity. Journal of anatomy. 2015 Oct:227(4):418-30. doi: 10.1111/joa.12361. Epub 2015 Aug 7 [PubMed PMID: 26249743]
Cole P, Kaufman Y, Hatef DA, Hollier LH Jr. Embryology of the hand and upper extremity. The Journal of craniofacial surgery. 2009 Jul:20(4):992-5. doi: 10.1097/SCS.0b013e3181abb18e. Epub [PubMed PMID: 19553860]
Wilde S, Feneck EM, Mohun TJ, Logan MPO. 4D formation of human embryonic forelimb musculature. Development (Cambridge, England). 2021 Feb 17:148(4):. doi: 10.1242/dev.194746. Epub 2021 Feb 17 [PubMed PMID: 33234713]
Poirot Y, Duparc F, Hue AG, Gandolfi S, Dacher JN, Auquit-Aukbur I. Cutaneous vascularization of the proximal two-thirds of the dorsal aspect of the hand: descriptive anatomical study of a perforating arterial arch. Surgical and radiologic anatomy : SRA. 2023 Sep:45(9):1073-1081. doi: 10.1007/s00276-023-03185-w. Epub 2023 Jul 12 [PubMed PMID: 37438569]
Granoff MD, Pardo JA, Johnson AR, Fleishman A, Tillotson E, Thomson S, Lee BT, Singhal D. Superficial and Functional Lymphatic Anatomy of the Upper Extremity. Plastic and reconstructive surgery. 2022 Oct 1:150(4):900-907. doi: 10.1097/PRS.0000000000009555. Epub 2022 Aug 4 [PubMed PMID: 35939638]
Yang T, Rui YJ. Innervation of the lumbrical and interosseous muscles in hand: analysis of distribution of nerve fascicles and quantification of their surface projections. Journal of plastic surgery and hand surgery. 2022 Oct:56(5):310-317. doi: 10.1080/2000656X.2021.1981348. Epub 2021 Sep 28 [PubMed PMID: 34581658]
Chambers SB, Wu KY, Smith C, Potra R, Ferreira LM, Gillis J. Interfascicular Anatomy of the Motor Branch of the Ulnar Nerve: A Cadaveric Study. The Journal of hand surgery. 2023 Mar:48(3):309.e1-309.e6. doi: 10.1016/j.jhsa.2021.10.012. Epub 2021 Dec 20 [PubMed PMID: 34949481]
Eladoumikdachi F, Valkov PL, Thomas J, Netscher DT. Anatomy of the intrinsic hand muscles revisited: part I. Interossei. Plastic and reconstructive surgery. 2002 Oct:110(5):1211-24 [PubMed PMID: 12360058]
Nayak VS, Priya A, Bhat N, Nayak SS, D'Souza AS, Bangera H, Sumalatha S. Cadaveric Study on Morphology of Dorsal Interossei of Hand and its Anatomical Variation. Journal of clinical and diagnostic research : JCDR. 2016 Jun:10(6):AC04-6. doi: 10.7860/JCDR/2016/19068.8034. Epub 2016 Jun 1 [PubMed PMID: 27504270]
Fatima A, Ahmed O, Ahmed M, Beg MSA, Batool A, Siddiqui MM. Metacarpal Fractures, Management Techniques, and Outcomes in Our Center. Cureus. 2021 Sep:13(9):e17828. doi: 10.7759/cureus.17828. Epub 2021 Sep 8 [PubMed PMID: 34660037]
Mejia A, Lichtig AE, Ghosh A, Balasubramaniyan A, Mass D, Amirouche F. The Effect of Metacarpal Shortening on Finger Strength and Joint Motion: A Cadaveric Biomechanical Study. Journal of hand surgery global online. 2023 Jul:5(4):407-412. doi: 10.1016/j.jhsg.2023.03.007. Epub 2023 Apr 6 [PubMed PMID: 37521540]
Abdul-Hamid AK. First dorsal interosseous compartment syndrome. Journal of hand surgery (Edinburgh, Scotland). 1987 Jun:12(2):269-72 [PubMed PMID: 3624994]
Level 3 (low-level) evidenceAndrews K, Rowland A, Pranjal A, Ebraheim N. Cubital tunnel syndrome: Anatomy, clinical presentation, and management. Journal of orthopaedics. 2018 Sep:15(3):832-836. doi: 10.1016/j.jor.2018.08.010. Epub 2018 Aug 16 [PubMed PMID: 30140129]
Vij N, Traube B, Bisht R, Singleton I, Cornett EM, Kaye AD, Imani F, Mohammadian Erdi A, Varrassi G, Viswanath O, Urits I. An Update on Treatment Modalities for Ulnar Nerve Entrapment: A Literature Review. Anesthesiology and pain medicine. 2020 Dec:10(6):e112070. doi: 10.5812/aapm.112070. Epub 2020 Dec 24 [PubMed PMID: 34150581]