 Anatomy, Shoulder and Upper Limb: Hand Anatomical Snuff Box
Anatomy, Shoulder and Upper Limb: Hand Anatomical Snuff Box
Introduction
The anatomical snuffbox is a surface anatomy feature described as a triangular depression on the dorsum of the hand at the base of the thumb (see Image. Hand Anatomical Snuffbox). This depression becomes prominently visible with ulnar deviation of the wrist and abduction and extension of the thumb. The term “snuffbox” originates from the historical use of this area as a site for inhaling powdered tobacco, or dry snuff. The anatomical snuffbox appeared in surgical anatomy texts prior to 1850. Further elaboration of the region was provided in 19th-century works by anatomists such as Germain Cloquet and Marie-François Bichat. Widespread inclusion of the anatomical snuffbox in formal anatomical textbooks followed in the early 20th century.[1][2]
The anatomical snuffbox is bordered medially by the tendon of the extensor pollicis longus (EPL) and laterally by the tendons of the extensor pollicis brevis (EPB) and abductor pollicis longus (APL). The floor of this region consists of the scaphoid and trapezium bones, as well as the tendons of the extensor carpi radialis longus and extensor carpi radialis brevis. Palpable landmarks within the snuffbox include the styloid process of the radius proximally and the base of the 1st metacarpal bone distally. Structures contained within this region include the radial artery, the superficial branches of the radial nerve, and the cephalic vein.[3]
The anatomical snuffbox holds clinical relevance because the scaphoid bone, located at the floor of the snuffbox, is readily accessible to palpation (see Image. Scaphoid Bone of the Wrist). Following trauma, tenderness in this location may indicate a scaphoid fracture. Missed or delayed diagnosis of such a fracture may result in chronic pain and long-term functional impairment.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The anatomical snuffbox is a broadly triangular, superficial depression in the skin that becomes apparent when the thumb is held in abduction and the wrist in ulnar deviation. The base of the anatomical snuffbox aligns with the radial styloid process, while the apex points distally toward the 1st metacarpophalangeal (MCP) joint.
Viewed from above, the medial (ulnar) boundary of the anatomical snuffbox is defined by the tendon of the EPL. The lateral (radial) boundary is formed by the parallel-running tendons of the EPB and the APL (see Image. Anatomical Snuff Box and Ulnar Styloid Process).
The EPL originates from the midshaft of the ulna and inserts into the base of the distal phalanx of the thumb, serving as the principal extensor of the terminal phalanx. This muscle receives innervation from the posterior interosseous nerve (PIN).[4]
The EPB and the APL both originate from the posterior surfaces of the radius and ulna. The EPB is more closely associated with the radius and the interosseous membrane.[5] The APL inserts via 2 tendinous slips: one at the base of the 1st metacarpal and another at the trapezium. The EPB inserts as a slender tendon at the base of the proximal phalanx of the thumb. Both the APL and EPB are innervated by the PIN. Functionally, both muscles extend the thumb at the carpometacarpal joint, and the EPB additionally extends the thumb at the MCP joint.
The base of the anatomical snuffbox contains several palpable bony landmarks. From proximal to distal, these landmarks include the radial styloid process, the scaphoid, the trapezium, and the base of the 1st metacarpal. These structures can be identified on examination with the hand placed in ulnar deviation and the thumb fully extended.[6]
Although the anatomical snuffbox is a surface anatomy feature, it gains clinical relevance through its spatial relationships with deeper structures. Accurate identification of its boundaries and contents allows the healthcare provider to formulate a differential diagnosis when evaluating localized pain. For instance, tenderness within the anatomical snuffbox following a fall on an outstretched hand suggests a scaphoid fracture, which requires further evaluation through radiographic imaging to confirm the diagnosis. Familiarity with the structures traversing this region also benefits vascular access procedures, particularly in patients with difficult peripheral access, because both the radial artery and the cephalic vein lie within the confines of the anatomical snuffbox.[7]
Blood Supply and Lymphatics
The anatomical snuffbox does not possess an independent blood supply, but several vessels traverse its boundaries. The cephalic vein and the radial artery both course through this region. Among these vessels, branches of the radial artery are most clinically significant due to their role in supplying the scaphoid bone. Approximately 80% of the proximal scaphoid receives blood via intraosseous retrograde flow from direct branches of the radial artery that enter through the articular foramina. The remaining perfusion is provided by volar scaphoid branches of the radial artery that enter at the distal pole. This retrograde vascular pattern predisposes the scaphoid to avascular necrosis, particularly following fractures that disrupt the arterial inflow within the anatomical snuffbox.[8]
Nerves
The superficial branches of the radial nerve that course through the anatomical snuffbox can be palpated and occasionally rolled over the tendon of the EPL, which defines the medial border of the snuffbox.[9] These sensory branches belong to the superficial branch of the radial nerve, which is this nerve's terminal division. The radial nerve arises from the posterior cord of the brachial plexus and receives contributions from nerve roots C5 to C8 and T1.
The radial nerve's course begins in the axilla and continues distally along the upper limb. The nerve passes between the long and medial heads of the triceps brachii, wraps around the posterior aspect of the humerus in a spiral trajectory, and pierces the lateral intermuscular septum approximately 1/3 of the way down the arm. As the nerve descends into the forearm, it gives rise to the PIN (C7, C8), which is its final motor branch.
The remaining fibers continue as the superficial branch of the radial nerve. This slender sensory branch travels along the lateral aspect of the forearm and enters the anatomical snuffbox, where it provides cutaneous innervation to the dorsum of the radial 2 1/2, as well as the adjacent dorsal surface of the hand (see Image. Cutaneous Innervation of the Right Upper Extremity).[10]
Muscles
The anatomical snuffbox is bordered medially by the tendon of the EPL and laterally by the tendons of the EPB and the APL. Both the EPB and the APL contribute to thumb extension, producing movement in the lateral horizontal plane.[11][12] The APL acts primarily at the carpometacarpal joint, while the EPB functions at both the carpometacarpal and MCP joints. The floor of the anatomical snuffbox is partially formed by the tendons of the extensor carpi radialis longus and the extensor carpi radialis brevis.[13]
Physiologic Variants
Anatomical research has identified multiple variations in the tendons associated with the anatomical snuffbox. Both the EPL and the APL may present with supernumerary tendon slips and atypical insertion sites. These variations hold clinical relevance, as certain configurations may predispose patients to tendinopathy involving either muscle. Tendon variability also has implications for surgical planning, particularly when operative intervention is considered for tendon pathology or trauma.[14]
Cadaveric studies have similarly documented variations in the course of the cephalic vein and the radial artery within the anatomical snuffbox. These findings are clinically significant in the context of intravenous cannulation or vascular access, which may be attempted in this region. Anomalous vascular anatomy increases the risk of inadvertent arterial puncture, potentially resulting in pseudoaneurysm formation, arterial occlusion, or localized hematoma.[15]
Surgical Considerations
The superficial branch of the radial nerve is the 3rd most frequently injured peripheral nerve. Damage to this branch produces paresthesia over the dorsum of the 1st webspace of the hand. Awareness of the nerve's variable course within the anatomical snuffbox is essential during surgical procedures to prevent iatrogenic injury.
The anatomical snuffbox also serves as an alternative access point for percutaneous arterial entry during coronary intervention.[16][17] This approach offers several advantages over the conventional radial artery puncture. Most notably, collateral perfusion from the proximal radial artery remains intact in the event of complete arterial occlusion by the angiography catheter, thereby minimizing the risk of hand ischemia. Bleeding complications or localized subcutaneous hematomas arising from this access point are often controlled directly within the snuffbox, without the need for circumferential wrist compression. In contrast to traditional radial access, this technique preserves wrist mobility and improves patient comfort during the postprocedural period.
The conventional radial artery approach remains a reliable alternative if arterial access via the anatomical snuffbox is not feasible, or complications such as vasospasm or hemorrhage arise following successful cannulation. A limitation of snuffbox access is the relatively small caliber of the radial artery in this region. Despite this anatomical constraint, a cohort study reported successful cannulation using a 6 Fr catheter in 132 of 150 patients. Based on these findings, the authors concluded that anatomical snuffbox access is both feasible and safe for coronary angiography and percutaneous coronary intervention.[18]
Clinical Significance
The anatomical snuffbox holds clinical relevance when palpation within its boundaries elicits pain. Scaphoid fractures represent approximately 2/3 of all carpal bone fractures and are frequently misdiagnosed. The most common mechanism of injury involves a fall onto an outstretched hand positioned in pronation and ulnar deviation.
Tenderness within the anatomical snuffbox is a hallmark finding and demonstrates high sensitivity for scaphoid fractures, although specificity is limited. Patients with snuffbox tenderness should undergo radiographic evaluation of the wrist because of this limitation. In cases where initial imaging is negative, management may include immobilization with a short-arm thumb spica splint or further evaluation using advanced imaging tools, such as magnetic resonance imaging or computed tomography, to confirm or exclude fracture. Due to the scaphoid’s retrograde blood supply, the fracture location significantly influences treatment decisions and the risk of avascular necrosis.[19]
Accurate diagnosis of scaphoid fractures is essential, as up to 32% of cases progress to nonunion, ultimately resulting in osteoarthritis.[20] Failure to identify and treat this fracture can have significant and lasting consequences for a patient's quality of life. In cases of nondisplaced or minimally displaced scaphoid fractures, a systematic review and meta-analysis of available studies found no significant difference in long-term pain or disability outcomes between operative and nonoperative treatment strategies.[21]
De Quervain tenosynovitis is another clinically relevant condition associated with the anatomical snuffbox. This stenosing tendinopathy affects the 1st dorsal compartment, which contains the APL and the EPB, both of which form the lateral border of the anatomical snuffbox. Diagnosis is based on clinical history and physical examination.
Affected individuals often report repetitive wrist motion, particularly involving repeated radioulnar deviation. Common clinical findings include pain and localized swelling over the dorsolateral aspect of the wrist, with symptom provocation during resisted thumb extension or abduction. Initial management involves conservative therapy, including nonsteroidal anti-inflammatory drugs, corticosteroid injections, physical therapy, or immobilization using a thumb spica splint. Surgical release is reserved for cases with persistent symptoms despite conservative treatment.[22]
Media
(Click Image to Enlarge)

Cutaneous Innervation of the Right Upper Extremity. This image shows the sensory distribution of peripheral nerves in the right upper limb. Each colored region corresponds to the cutaneous territory of a specific nerve. The areas innervated by the radial nerve are shaded pink, covering portions of the posterior arm, forearm, and dorsolateral hand. Anterior and posterior views illustrate contributions from the cervical and thoracic spinal nerves via named cutaneous branches.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
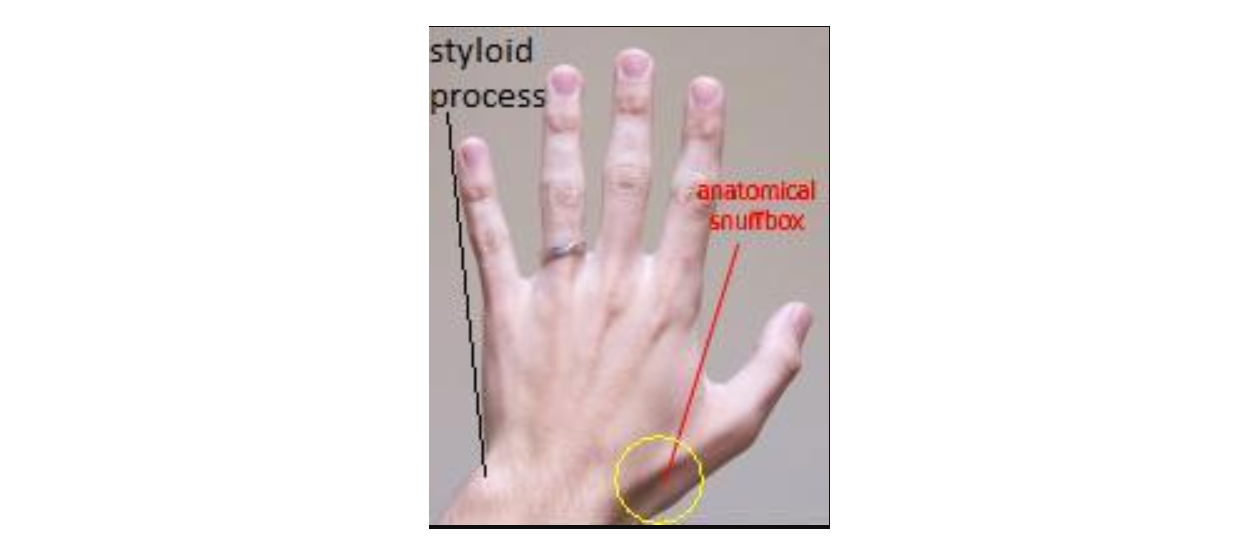
Anatomical Snuff Box and Ulnar Styloid Process. The anatomical snuff box and ulnar styloid process are shown in the image. The boundaries of the anatomical snuff box are the tendons of the abductor pollicis longus and extensor pollicis brevis laterally and the extensor pollicis longus medially.
Mcstrother, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
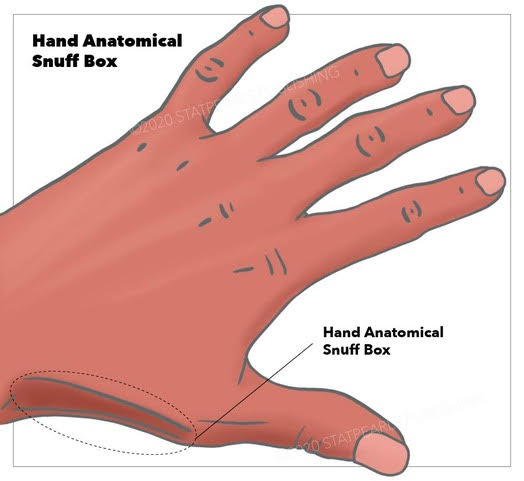
Hand Anatomical Snuffbox. Illustration of the left hand in pronation, highlighting the surface anatomy of the anatomical snuffbox along the radial aspect of the wrist.
StatPearls Publishing
(Click Image to Enlarge)

Scaphoid Bone of the Wrist. This image highlights the scaphoid bone (red arrow) on the lateral side of the wrist. Positioned between the radius and the base of the thumb, the scaphoid supports wrist stability and is prone to fractures. The scaphoid is the most frequently injured among the carpal bones.
Contributed by S Munakomi, MD
References
Sapundzhiev N, Werner JA. Nasal snuff: historical review and health related aspects. The Journal of laryngology and otology. 2003 Sep:117(9):686-91 [PubMed PMID: 14561353]
Seidenberg AB, Halperin EC, Goldstein AO. It's time to snuff out the "anatomical snuff box". Academic medicine :, journal of the Association of American Medical Colleges... 2015 Aug:90(8):1003-4. doi: 10.1097/ACM.0000000000000784. Epub [PubMed PMID: 26218360]
Berger RA. The anatomy of the scaphoid. Hand clinics. 2001 Nov:17(4):525-32 [PubMed PMID: 11775465]
Strauch RJ, Strauch CB. Extensor pollicis brevis tendon can hyperextend thumb interphalangeal joint in absence of extensor pollicis longus: Case report and review of the literature. World journal of orthopedics. 2016 Jul 18:7(7):448-51. doi: 10.5312/wjo.v7.i7.448. Epub 2016 Jul 18 [PubMed PMID: 27458556]
Level 3 (low-level) evidenceShigematsu S, Shimizu H, Beppu M, Hirata K. Anatomy of the extensor pollicis brevis associated with an extension mechanism of the thumb metacarpophalangeal joint. Hand surgery : an international journal devoted to hand and upper limb surgery and related research : journal of the Asia-Pacific Federation of Societies for Surgery of the Hand. 2014:19(2):171-9. doi: 10.1142/S0218810414500166. Epub [PubMed PMID: 24875499]
Roh JH, Lee JH. Distal Radial Approach through the Anatomical Snuff Box for Coronary Angiography and Percutaneous Coronary Intervention. Korean circulation journal. 2018 Dec:48(12):1131-1134. doi: 10.4070/kcj.2018.0293. Epub [PubMed PMID: 30403016]
Sendher R, Ladd AL. The scaphoid. The Orthopedic clinics of North America. 2013 Jan:44(1):107-20. doi: 10.1016/j.ocl.2012.09.003. Epub [PubMed PMID: 23174330]
Gelberman RH, Menon J. The vascularity of the scaphoid bone. The Journal of hand surgery. 1980 Sep:5(5):508-13 [PubMed PMID: 7430591]
Robson AJ, See MS, Ellis H. Applied anatomy of the superficial branch of the radial nerve. Clinical anatomy (New York, N.Y.). 2008 Jan:21(1):38-45 [PubMed PMID: 18092362]
Gurses IA, Coskun O, Gayretli O, Kale A, Ozturk A. The relationship of the superficial radial nerve and its branch to the thumb to the first extensor compartment. The Journal of hand surgery. 2014 Mar:39(3):480-3. doi: 10.1016/j.jhsa.2013.12.004. Epub 2014 Feb 1 [PubMed PMID: 24495622]
Öztürk K, Dursun A, Kastamoni Y, Albay S. Anatomical variations of the extensor tendons of the fetal thumb. Surgical and radiologic anatomy : SRA. 2021 May:43(5):755-762. doi: 10.1007/s00276-020-02611-7. Epub 2020 Nov 10 [PubMed PMID: 33170332]
Sugiura S, Matsuura Y, Suzuki T, Nishikawa S, Mori C, Kuniyoshi K. Variant course of extensor pollicis brevis tendon in the third extensor compartment. Surgical and radiologic anatomy : SRA. 2018 Mar:40(3):345-347. doi: 10.1007/s00276-017-1923-y. Epub 2017 Nov 14 [PubMed PMID: 29138875]
Adams JE, Habbu R. Tendinopathies of the Hand and Wrist. The Journal of the American Academy of Orthopaedic Surgeons. 2015 Dec:23(12):741-50. doi: 10.5435/JAAOS-D-14-00216. Epub 2015 Oct 28 [PubMed PMID: 26510626]
Thwin SS, Fazlin F, Than M. Multiple variations of the tendons of the anatomical snuffbox. Singapore medical journal. 2014 Jan:55(1):37-40 [PubMed PMID: 24452976]
Lirk P, Keller C, Colvin J, Colvin H, Rieder J, Maurer H, Moriggl B. Unintentional arterial puncture during cephalic vein cannulation: case report and anatomical study. British journal of anaesthesia. 2004 May:92(5):740-2 [PubMed PMID: 15003983]
Level 3 (low-level) evidencePua U, Quek LHH. "Snuffbox" Distal Radial Access. Journal of vascular and interventional radiology : JVIR. 2018 Jan:29(1):44. doi: 10.1016/j.jvir.2017.07.011. Epub [PubMed PMID: 29258662]
Kiemeneij F. Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI). EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology. 2017 Sep 20:13(7):851-857. doi: 10.4244/EIJ-D-17-00079. Epub [PubMed PMID: 28506941]
Kim Y, Ahn Y, Kim I, Lee DH, Kim MC, Sim DS, Hong YJ, Kim JH, Jeong MH. Feasibility of Coronary Angiography and Percutaneous Coronary Intervention via Left Snuffbox Approach. Korean circulation journal. 2018 Dec:48(12):1120-1130. doi: 10.4070/kcj.2018.0181. Epub 2018 Aug 6 [PubMed PMID: 30088362]
Level 2 (mid-level) evidenceKo JH, Pet MA, Khouri JS, Hammert WC. Management of Scaphoid Fractures. Plastic and reconstructive surgery. 2017 Aug:140(2):333e-346e. doi: 10.1097/PRS.0000000000003558. Epub [PubMed PMID: 28746289]
Cohen A, Reijman M, Kraan GA, Mathijssen NMC, Koopmanschap MA, Verhaar JAN, Mol S, Colaris JW, SUSPECT study group. Clinically SUspected ScaPhoid fracturE: treatment with supportive bandage or CasT? 'Study protocol of a multicenter randomized controlled trial' (SUSPECT study). BMJ open. 2020 Sep 29:10(9):e036998. doi: 10.1136/bmjopen-2020-036998. Epub 2020 Sep 29 [PubMed PMID: 32994236]
Level 1 (high-level) evidenceLi H, Guo W, Guo S, Zhao S, Li R. Surgical versus nonsurgical treatment for scaphoid waist fracture with slight or no displacement: A meta-analysis and systematic review. Medicine. 2018 Nov:97(48):e13266. doi: 10.1097/MD.0000000000013266. Epub [PubMed PMID: 30508914]
Level 1 (high-level) evidenceAshurst JV, Turco DA, Lieb BE. Tenosynovitis caused by texting: an emerging disease. The Journal of the American Osteopathic Association. 2010 May:110(5):294-6 [PubMed PMID: 20538752]
Level 3 (low-level) evidence